Different regimen of catheter directed thrombolysis in a case of upper extremity deep vein thrombosis
Image Description
Acute upper extremity deep vein thrombosis (DVT) represents a rare condition cumulating 1 to 4 percent of all cases of DVT, with an estimated annual incidence of 1 to 2 cases per 100,000 population1. No treatment has been rigorously evaluated for upper extremity deep vein thrombosis. Besides anticoagulation to maintain patency of collateral veins and to reduce propagation of thrombus, thrombolysis and mechanical thrombectomy are other viable options but with low level of evidence2.
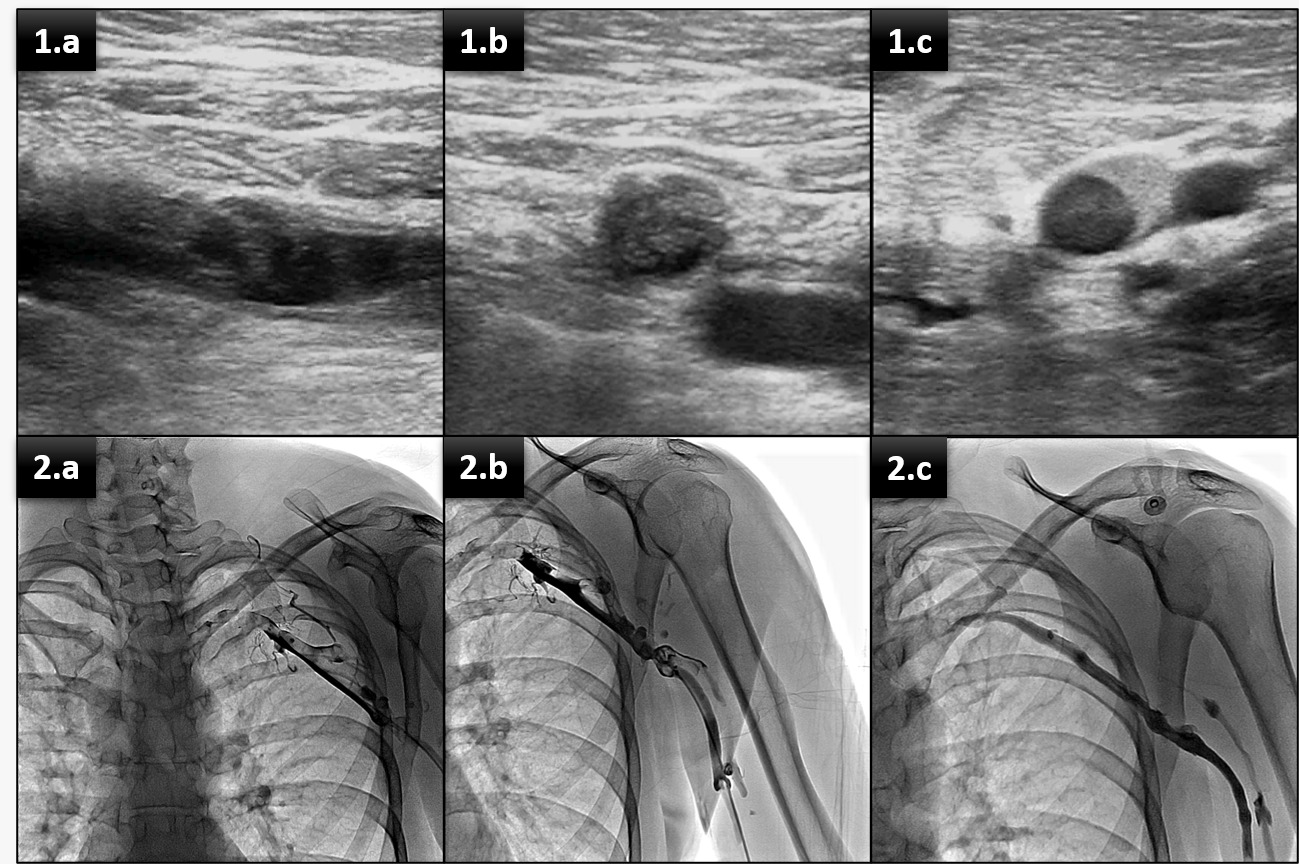
We present the case of a 33 years old male admitted to the Emergency Department with acute onset (24 hours) of upper extremity pain and swelling in the non-dominant arm. Emergency Doppler ultrasound showed occlusive thrombosis of the axillosubclavian vein (Figure 1.a and 1.b) extended to the distal portion of the brachial vein(Figure 1.c). Initially, the patient received anticoagulation with unfractionated heparin for 72 hours and systemic thrombolytic therapy with Alteplase (25mg over 12 hours - 0.04 mg/kg/hr) without results. Given the age of thrombus (>48 hours) and the lack of response to current therapy, the interventional radiology team decided that the best option is catheter-directed thrombolysis (Figure 2.a) with an attack dose of 25mg Alteplase over 30 minutes ( 1/4 of the recommended dose in pulmonary embolism). After that partial re-permeabilization (Figure 2.b) was seen. Given this result the catheter-directed thrombolytic therapy was continued for another 24 hours with 50mg Alteplase (0.04 mg/kg/hr) with complete re-permeabilization (Figure 3.b). The evolution of the patient was favorable, and no complications occurred during these procedures.
References
Mills JL. Primary ( spontaneous ) upper extremity deep vein thrombosis. Published online 2021:1-32.
Vineet Chopra, MD. Catheter-related upper extremity venous thrombosis. In: UpToDate, Collins, KA(Ed).2020